Topographic percussion of the anterior
a Lung-liver border
On the anterior aspect of the thorax only the right lung border can be determined. On the left-hand side this is not possible due to the position of the heart. Anteriorly, instead of an exact border, a transitional area is identified due to the presence of the liver arch.
This transitional area is indicated by a relative and absolute lung-liver border. The relative lung-liver border is the position where a clear, resonant tone suddenly becomes somewhat duller. At this position the upper border of the liver is located, but not the lower border of the lung. When determining the size of the liver, as part of the abdominal examination, this border is very important. When percussing downwards from this border, all resonance disappears at a certain point and the percussion tone becomes dull. This is the lower border of the lung, the absolute border that is normally present at the level of the fifth intercostal space. To count the intercostal spaces, the sternal angle (transition from manubrium to the body of the sternum) is used as a reference point. The second rib attaches at this position. Between the second and third rib the second intercostal space is found.
Procedure
Ask the patient to lie on their back. Then, with the fingers parallel to the ribs, percuss downwards along the midclavicular line. In men this is usually a vertical line through the nipple. In women, the breasts can hinder interpretation of the percussion tone. In such cases it is best to move the breast up with the pleximeter finger before percussing along the midclavicular line whilst gradually moving the finger downwards. Determine the relative and absolute lung-liver border as accurately as possible. Again, it is best to move the pleximeter finger only as much as one finger-width at a time when reaching the lung border; percussion can be continued normally across the ribs [Figure 27a and 27b].
 Figure 27a: Percussion of the lung-liver border
Figure 27a: Percussion of the lung-liver border
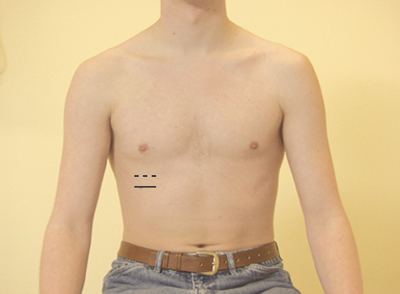 Figure 27b: The lung-liver border
Figure 27b: The lung-liver border
– – – = relative lung-liver border
____ = absolute lung-liver border
b Heart borders
It is important to determine the area of cardiac dullness during the lung examination since, given the position of the heart, it is the only area of the mediastinum that can be percussed and that can therefore give an indication of any intrathoracic abnormalities. Mediastinal displacement could fit with a number of conditions, including (tension) pneumothorax or atelectasis in one of the lower fields. Absence of cardiac dullness indicates that there is a layer of lung tissue at least 5 cm thick in front of the heart. This is observed in the case of over-inflated lungs, as seen with pulmonary emphysema. As with the liver, during percussion of the heart transitional areas are found with resonant and dull elements present in the percussion tone. This provides a global impression of the position of the heart.
Three different borders can be determined using percussion:
- the right border. This is usually found at the level of the right parasternal line.
- the left border. This is usually found 1 to 2 cm medially to the midclavicular line.
- the upper border. This border should be approximately at the level of the third intercostal space.
Procedure
- Determine the right heart border by percussing in a slight upwards direction from the lung-liver border with the pleximeter finger placed vertically, and moving from right to left.
- Determine the left heart border by percussing at the same level from the left anterior axillary line with the pleximeter finger placed vertically or horizontally and moving towards the right.
- Determine the upper border of the heart by percussing from the left midclavicular line in a downwards and medial direction [Figures 28a and 28b] with the pleximeter finger placed perpendicular to the direction of percussion.
 Figure 28a: heart borders
Figure 28a: heart borders
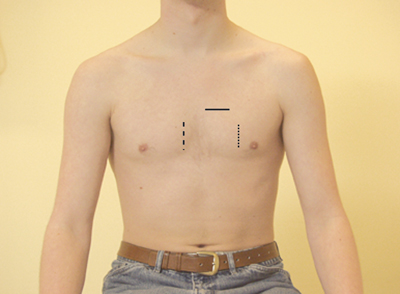 Figure 28b: percussion of the heart borders
Figure 28b: percussion of the heart borders
_____ = upper border of the heart
——– = right heart border
…….. = left heart border
c Traube’s space
Finally, Traube’s space can also be percussed. This is the area on the thorax where tympanic percussion is audible. The fundus of the stomach is located in this area. Traube’s space is bordered by the heart, the liver and the spleen. If one of these organs is enlarged, or when extensive pleural fluid is present, the tympanic percussion tone in this area disappears.
Procedure
Percuss Traube’s space and determine the nature of the percussion tone [Figure 29].
 Figure 29: Percussion of Traube’s space
Figure 29: Percussion of Traube’s space
Comparative percussion
Procedure
Start in the supraclavicular fossa. Percuss the ribs in a downwards direction with the pleximeter finger parallel to the ribs, always comparing left and right. Also percuss the clavicle without using the pleximeter finger, as well as the other areas, preferably in the intercostal spaces. Examine a larger area in the event of abnormal findings and try to mark the abnormal area [Figure 30].
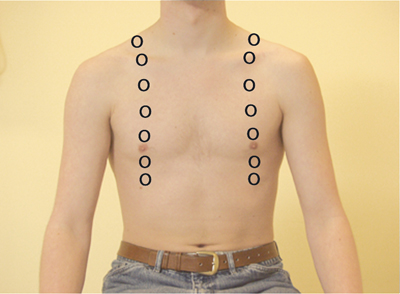 Figure 30: Percussion points for comparative percussion: anterior
Figure 30: Percussion points for comparative percussion: anterior



























