Topographic percussion
During topographic percussion of the posterior thorax, the locations of both the left and right lung boundaries are determined and compared to one another. The boundary is usually 1 to 2 cm higher for the right lung compared to the left lung due to the position of the liver. For correct interpretation and reporting, it is necessary to describe the location of the boundary using anatomical landmarks (i.e., the corresponding spinous process). Normally, the boundaries are located at approximately the height of the eleventh thoracic vertebra (T11). The spinous processes can be identified in a patient by first searching for the seventh cervical spinous process (C7): the vertebra prominens, which protrudes the most of all vertebrae in the cervical spine when a patient has the head bent forward. If two processes are equally protruding then these are usually C7 and T1; from C7, one can count downwards. In lean patients this can be done well with their back hunched. In a muscular or obese patient palpation is easier carried out with the patient in prone position because all back muscles will relax in this position. If either method fails then one can count from caudal to cranial. Here, a landmark line through both iliac crests should be used as the starting point. This method is less accurate since either L2 or L3 can be present on this line. In this manner, it is possible to determine whether the lung borders are positioned in more or less the right place.
Procedure
Have the patient sit on the examination table (preferably with legs hanging down). Allow the back to be slightly curved and the hands to be relaxed on the legs or on the examination table. Ask for assistance with very ill patients to have them placed temporarily in a seated position. Then, with the fingers parallel to the ribs, percuss along the scapular line in a caudal (downwards) direction. Determine as precisely as possible the transition from resonant to dull percussion and possibly mark this border with a skin marking pencil. It is best to move the finger only as much as one finger-width at a time when reaching the lung border. The ribs can be percussed as normal. Note the anatomical height of the identified border. Repeat the procedure on the other side. Finally, compare the findings [Figure 23]
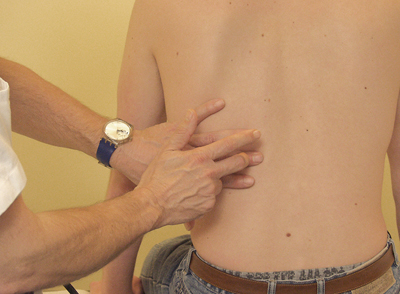 Figure 23; topographic percussion of the posterior thorax
Figure 23; topographic percussion of the posterior thorax
Examination of the mobility of the lung borders, before and after maximum inspiration
The normal mobility of the lung borders is approximately two finger widths or 4-6 cm.
A reduction in respiratory mobility is part of the physiological ageing process and can also occur in disorders such as muscle weakness and emphysema.
Procedure
Ask the patient to breathe normally. Percuss one of the two posterior lung boundaries and, if desired, use a skin pencil to mark these by drawing a horizontal line at the point where the resonant percussion turns to dull percussion. Place the pleximeter finger on the point where a dull tone was first heard (i.e. just below the lung border). Then, ask the patient breath in as deeply as possible and hold their breath for a short period.
Now percuss in a downwards direction and again note the upper border where a dull tone is first heard. Ask the patient to resume normal breathing and report the measured mobility in centimetres or finger-widths. Repeat this procedure for the mobility of the lung border on the other side of the thorax [Figure 24].
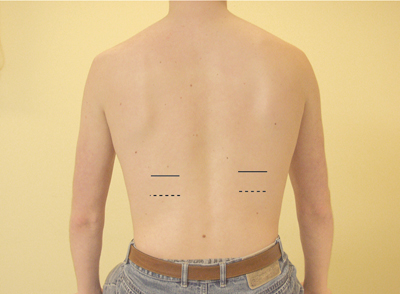 Figure 24: Topographicpercussion of the posterior thorax and the examination of the lung mobility
Figure 24: Topographicpercussion of the posterior thorax and the examination of the lung mobility
____ = lung borders during normal breathing
——- = lung borders during maximal breathing
With abnormal findings a more detailed examination is possible by carrying out percussion of respiratory mobility along the midaxillary line on the left and right sides.
If there is a complete absence of respiratory mobility, the presence of paradoxical movement of the diaphragm can be investigated. This only occurs with phrenic nerve paralysis (paralysis of the nerve that innervates the diaphragm). With this, upon deep inspiration the diaphragm rises instead of descends. During paradoxical movement the percussion tone changes from resonant at steady breathing to dull during deep breathing. By subsequently percussing in an upwards direction, rather than downwards, during deep inspiration, the (degree of) upwards displacement of the lung can be detected.
Comparative percussion
Procedure
Start above the lung apices, working downwards and always comparing left and right. Circumvent the scapula in an ‘S’-shaped Figure and then continue along the scapular line. Examine a larger area in the event of abnormal findings and try to mark the abnormal area [Figure 25]
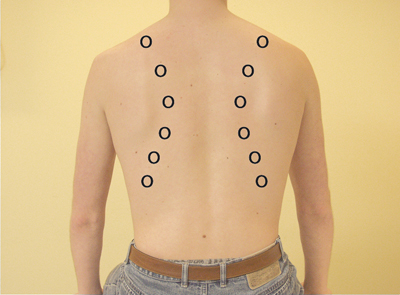 Figure 25: Percussion points for comparative percussion: posterior
Figure 25: Percussion points for comparative percussion: posterior



























