Foetal growth cannot be accurately determined by means of an external examination. The fundal height of the uterus can, however, give a good impression of growth. As the pregnancy advances, the growing foetus becomes more of a determining factor for the intra-uterine volume increase than the placenta and amniotic fluid, as a result of which the foetus can be assessed more accurately.
However, the importance of the fundal measurement has more to do with determining the extent of growth (the difference between two measurements) than in determining the duration of the pregnancy.
The fundal height can be determined on the basis of the reference points: symphysis (s), navel (n) and xiphoid process (x) [Figure 13].
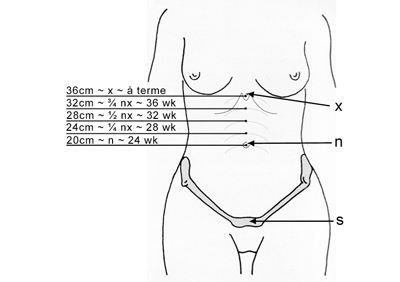 Figure 13
Figure 13
The fundal measurement under the navel is not reliable. During the first half of the pregnancy, the size of the uterus can only be determined with a reasonable degree of accuracy by means of a bimanual examination.
At 20 weeks of amenorrhoea, the fundal height should be about 2/3 of the s-n distance, and at 24 weeks it should reach the navel (in the case of a single pregnancy). Subsequently, every four weeks, a quarter of the n-x distance is bridged. In the 36th week, the fundal height will therefore be at 3/4 of the n-x line. If the head engages after this time (in the case of some primigravida), there will be very little increase in fundal height in the remaining four weeks.
The accuracy of the estimation is strongly dependent on a number of factors, such as obesity, the position of the navel, the shape of the uterus (arcuate uterus, fibroids), the volume of amniotic fluid and the presentation of the foetus. The distance before the upper edge of the symphysis to the highest point of the fundus of the uterus can also be taken as a measure of the growth.
Above the navel, the distance from the symphysis to the highest point of the fundus corresponds in centimetres +4, with the amenorrhoea duration in weeks. Therefore, at a pregnancy duration of 34 weeks, a symphysis-fundus distance of 30 cm is expected. As the point where the measurement begins, there is skin over the symphysis which can shift. It is therefore advisable to measure the distance between the symphysis and navel as well. If this distance is the same as during the previous check-up, the fundal height measurement is reliable.
Procedure
- Ensure that the woman is lying in a relaxed supine position, her legs slightly flexed, with a pillow under her head and her arms at her side.
- Stand to the right of the woman facing her head, and place your hands on both sides of the fundus of the uterus.
- If necessary, first centre the uterus.
- With the ulnar side of the hands, determine the upper boundary of the uterus; avoid indenting or pushing down the uterus (first part of the first Leopold’s manoeuvre) [Figure 14].
 Figure 14
Figure 14
- Note your findings using the orientation points symphysis (s), navel (n) and xiphoid process (x).
- Next, palpate the upper side of the symphysis and lay a measuring tape from this point (the symphysis) over the navel to the upper edge of the fundus [Figure 15].
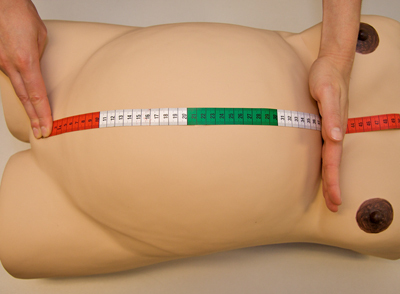 Figure 15
Figure 15
- Measure the symphysis-navel and symphysis-fundus distance in centimetres.
- Compare the findings with those from the previous examination.
If the fundal height is higher than expected based on the duration of amenorrhoea (size-dates ratio), it is known as large for gestational age (LGA). Causes of this are multiple pregnancy, a large child (diabetes mellitus), a large volume of amniotic fluid, a large placenta or a miscalculation in determining the duration of the pregnancy.
Small for gestational age (SGA) (uterus too small for the duration of pregnancy) can occur in the case of placental insufficiency, low amniotic fluid level or congenital abnormalities of the foetus. Once again, a miscalculation of the duration of pregnancy needs to be excluded, e.g. as a consequence of inaccurate recording of the cycle history (see “First check-up – history-taking”).



























