The kidneys are located behind the abdominal cavity (retroperitoneally) [Figures 36, 37]. Only a small portion of the ventral side of the kidneys is covered by the peritoneum. The right kidney normally lies somewhat lower than the left kidney. The upper portion of the kidneys is in close contact with the posterior portion of the diaphragm. As a result, renal disorders can cause deep abdominal pain or more localised pain in the back or side. The pain may radiate downward toward the groin. Shoulder pain can also occur (irritation of the diaphragm). Given that the kidneys lie close to the iliopsoas muscle, inflammation can cause reactive hypertonia in this muscle (walking with the head bent forward, positive psoas phenomenon).
 Figure 36: Projection of the kidneys on abdominal wall
Figure 36: Projection of the kidneys on abdominal wall
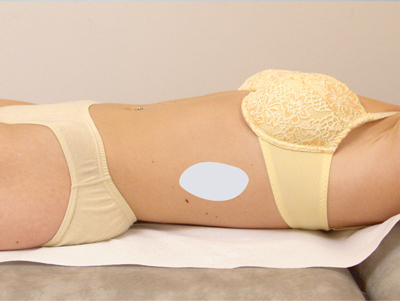 Figure 37: Projection of kidney in flank
Figure 37: Projection of kidney in flank
Normally, the kidneys are impalpable. Incidental palpation is only possible in slender adults with less developed abdominal muscles; in this case, it is often only the lower pole that can be felt. This means that physical diagnostic examination will provide no information on a normal kidney. Physical examination will reveal abnormalities in both kidney regions only in cases of markedly enlarged kidneys (e.g. polycystic kidneys) or inflammation of the kidney region. Most renal disorders are not detectable by physical examination.
General
For suspected kidney disorders, it is important to measure blood pressure and determine whether the patient has peripheral or pulmonary oedema. If hypertension is found, auscultation above the renal arteries can be performed [Figure 38] to detect signs of renal artery stenosis.
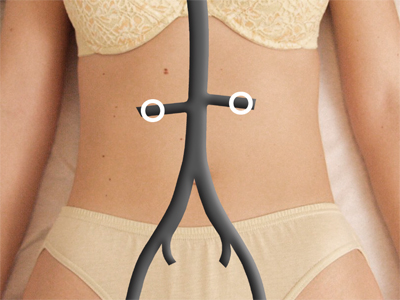 Figure 38: Auscultation points for renal arteries
Figure 38: Auscultation points for renal arteries
Percussion
If percussion reveals abnormal dullness in the left or right lateral region of the abdomen, it may indicate an enlarged kidney, although this is rare. Give extra attention to the kidneys during further examination.
Palpation
Routine palpation of the kidneys as described below is not beneficial. This examination should only be considered if the history-taking, another physical examination or additional tests suggest renal disorders. For example, if abdominal palpation reveals a tumour in the left or right upper abdomen, it should be considered whether this may be an enlarged kidney (usually a polycystic kidney, sometimes congenital or due to prolonged urinary flow obstruction). Application of the palpation techniques described below can further clarify these findings.
Procedure
Examination of the right kidney
- Lay your left hand flat on the right lumbar region between the costal arch and the iliac crest. The fingertips should lie approximately on the lateral border of the right quadratus lumborum muscle.
If necessary, this hand can be used to exert light upward pressure to raise and hold the right lumbar region in a slightly higher position. This can facilitate palpation. - Carefully lay your right hand flat on the upper right abdomen parallel to the costal arch and above the left hand.
- Ask the patient to breathe normally through the mouth.
- At each expiration of the patient, push the spread fingers of the right hand slowly and gradually towards the left hand. Stop at the point where it is no longer possible to go deeper, or when it becomes painful [Figure 39].
 Figure 39
Figure 39
- Maintain pressure on the kidney region and ask the patient to inhale as deeply as possible and then hold their breath.
During deep inspiration, the kidneys are displaced maximally in a caudal direction due to the contracting diaphragm. The chance of capturing the right kidney between both hands is greatest while the patient is holding their breath. - If a palpable mass is detected between the hands, it may be the kidney. Assess the mass quickly so that the patient does not have to hold their breath too long.
- Let the patient exhale (if they have not done so already). It is possible that the palpable mass will slip between the hands to resume its original position.
- Describe the findings carefully.
Examination of the left kidney
- Remain seated to the right of the patient or stand if necessary.
- Lay the left hand flat on the left lumbar region between the costal arch and the iliac crest. The fingertips should lie approximately on the lateral edge of the left quadratus lumborum muscle.
If necessary, this hand can be used to exert upward pressure to raise and hold the left lumbar region in a slightly higher position. This can facilitate palpation [Figure 40].
 Figure 40
Figure 40
- Carefully lay your right hand flat on the upper left abdomen parallel to the costal arch and exactly above the left hand.
The hand should point in the same direction as when palpating the right kidney. - Ask the patient to breathe normally through the mouth.
- Follow the same procedure as described for palpation of the right kidney.
Focus points
If a palpable mass is detected, assess its size, consistency (varying from soft to very firm), surface (varying from smooth to irregular and bumpy), palpation tenderness (under normal conditions, the kidneys are not painful to palpation).
Upon expiration, you may feel the kidneys slip between the hands.
Determining costovertebral angle percussion tenderness
A specific type of percussion is percussion to assess costovertebral angle tenderness.
Procedure 1
- Have the patient sit upright or stand.
- Sit or stand behind the patient.
- Give a short, strong blow [Figure 41] to the right costovertebral angle using the ulnar side of the outstretched hand. The hand should be held horizontally. Repeat for the left side.
Do not strike the patient hard. This will always cause pain. - Ask the patient if they felt a deep, dull pain (visceral pain); if so, ask whether there was a difference in pain between the left and right sides.
 Figure 41
Figure 41
Focus points
A patient who feels pain or worsening of pain on percussion of the costovertebral angle may have inflammation in the kidney region.
Procedure 2
A second procedure to provoke pain in the costovertebral angle is as follows:
- Lay one hand on the lumbar region adjacent to the costal arch.
- Make a fist with the other hand [Figure 42] and give a short, firm blow using the ulnar side to the opposite hand.
Do not strike the patient hard. This will always cause pain. - Repeat the same procedure on the right side.
- Ask the patient whether they felt a deep, dull pain; if so, ask whether there was a difference in pain between the left and right sides.
 Figure 42
Figure 42
Focus points
A patient who feels pain or worsening of pain during costovertebral angle percussion may have inflammation in the kidney region.



























